The Inconvenient Truth About Advocacy Disguised as Analysis
The Curious Case of Laura Targownik
There is a curious form of intellectual dishonesty that reveals itself not in what someone says, but in the distance between what they have said and what they are doing. It is the dishonesty of someone who knows better but has decided that knowing better does not serve their interests. The sort of thing we tell ourselves in order to convince ourselves, as much as our conservative family and friends, that we are not "that kind of gay" or "one of the those trans." We are the reasonable ones. The ones who understand. The ones who can be trusted. And in that reassurance lies a small compromise. Then another. Then another. Until the distance between what we know and what we are doing becomes a chasm we have stopped examining.
Within this philosophical musing lies this article which examines Dr. Laura Targownik's recent work on gender-affirming medical care.
Dr. Laura Targownik is a gastroenterologist and epidemiologist at the University of Toronto. She completed medical school in 1997, transitioned in 2000, and has built a 26-year career in digestive disease research. Her published work, over 450 peer-reviewed articles, focuses on inflammatory bowel disease and healthcare utilization. She has no published research on gender-affirming medical care, no clinical work with transgender youth, and no formal training in gender medicine.
She writes a blog hosted on Substack called "The Data-Driven Transsexual" and co-hosts a podcast on Youtube called "Agree to Disagree About Gender," with Yvette Nary, a "Gender Critical" activist, where they platform and interview almost exclusively folks critical of various aspects surrounding trans healthcare, or hold anti-trans views. She is quite the active Twitter user.
Targownik self-describes as “a binary assimilationist transsexual," a “pragmatic progressive,” and a transmedicalist. She has become increasingly involved publicly in trans politics since Trump's election in 2024.
In June 2026, she published "What Oregon Can Teach Canada About Pediatric Gender Medicine." This article recommends psychotherapy as first-line treatment, raises concerns about rising prevalence among AFAB youth, emphasizes the irreversibility of testosterone, and frames informed consent models with skepticism.[1]
What follows is an in-depth examination of that article: the evidence it cites, what that evidence actually shows, and what patterns emerge when we look carefully at how she has presented her case.
Follow the Academic Citations
Targownik cites researcher Kinnon MacKinnon's work on detransition, writing that MacKinnon has "suggested, as an informed estimate rather than a settled empirical finding, that 5% to 10% of this cohort may eventually detransition in adulthood."[1]
This framing is misleading on multiple counts. To understand why, we need to trace what MacKinnon is actually citing.
The Boyd/Hackett/Bewley Audit
MacKinnon's detransition estimates are drawn from two primary sources. The first is a UK primary care audit by Boyd, Hackett, and Bewley, published in 2022. This study examined 68 patients identified as trans or gender-diverse from a single GP practice in a remote part of Britain - 0.34% of that practice's total patient population. Of those 68 patients, only 41 had received hormone treatment. Of those 41, the study identified 4 with notes referencing detransition or a change in gender identity, yielding a 9.8% detransition rate.[2]
But read the study's own limitations: the researchers acknowledge that 29% of their identified patients had not yet been referred to a gender identity clinic. Without contacting these patients, they could not determine if they were pursuing transition or not. They note their small sample size from a single remote practice limits what we can confidently conclude applies elsewhere, including the detransition rate. They performed no statistical significance testing. This was a quality improvement audit conducted at one primary care practice, not a population epidemiological study. The methodology itself precludes drawing broad conclusions.
What MacKinnon does not disclose, and what Targownik certainly does not, is that two of the three authors of this methodologically limited study are embedded in anti-transgender activist organizations. Susan Bewley is an obstetrician and long-time anti-transgender activist who has published papers critical of trans healthcare terminology and protocols, speaks at anti-trans conferences organized by Society for Evidence-based Gender Medicine a.ka. SEGM (a known anti-trans hate group), and collaborates with organizations explicitly opposed to gender-affirming care.[3] Thomas Hackett and Isabel Boyd are listed as affiliates of the Detrans Foundation, an "ex-trans" foundation with similar underpinnings as the "ex-gay" movement.[4] The study that MacKinnon cites for his detransition prevalence estimates was authored by anti-trans activists embedded in organizations dedicated to restricting gender-affirming care. Furthermore, we need to keep these numbers in perspective, as the study concerns four individuals, in one primary care practice, in a remote part of Britain. This is the sample from which a 9.8% detransition rate is derived, and what appears to be the figure that anchors the upper bound of MacKinnon's 5–10% estimate, which Targownik presents as "an informed estimate."
The Oslo Misconduct Finding
The second source MacKinnon cites is research by Anne Waehre and colleagues. In June 2026, contemporaneous with Targownik's June article, the Integrity Committee of the University of Oslo, Oslo University Hospital, and Akershus University Hospital found Waehre, Trond H. Diseth, and Cecilie Bjertness Nyquist guilty of research misconduct. The committee determined they had committed "serious violations of recognized research ethics standards" that were "grossly negligent" and constituted "scientific misconduct." The committee recommended two of their published articles be retracted and others be referred to the Norwegian Office of the Ombudsman for further investigation.[5]
Targownik does not mention that one of her key sources, research cited by MacKinnon to establish detransition prevalence, was found guilty of research misconduct or that the associated papers have been referred for further investigation.
The Waehre study, despite its serious ethical violations, actually undercuts the high-detransition narrative. Its data shows detransition is rare. The ethical violation (accessing data without consent) is real and serious, but it doesn't make the detransition rate higher or lower; if anything, the study's acknowledged underestimation problem means the real rate could be somewhat higher than 2.3%, but the Boyd audit's 9.8% is still the outlier driving MacKinnon's upper bound.
Targownik doesn't disclose either of these points. MacKinnon's two sources actually shows detransition is uncommon, meaning the 5–10% estimate is being pulled upward almost entirely by a 4-person sub-sample from a single remote GP practice staffed by anti-trans activists.
MacKinnon's Warnings, Omitted
When Targownik describes MacKinnon's detransition figures as his "informed estimate rather than a settled empirical finding," she is burying several critical facts. MacKinnon is not generating his own estimates. He is citing a quality-improvement audit from a single remote primary care practice with a sample of 41 hormone-treated patients, authored by anti-trans activists, and research by authors found guilty of research misconduct. He is speculating that the true detransition rate is "probably higher" based on these compromised sources. Targownik presents this cascade of methodological weakness, ideological positioning (based on the authors of the paper, and to a lesser degree, MacKinnon's own position), and ethical violation as though it constitutes reliable epidemiological data.
Moreover, Targownik omits MacKinnon's explicit warnings about how this research should be used. In the same article where he discusses detransition figures, MacKinnon writes with absolute clarity:
"Nothing in my team's research, or any other studies on detransition, should lead to the conclusion that policymakers ought to issue blanket bans on gender-affirming care or that health care providers should ever try to change a person's gender identity or expression by engaging in so-called conversion therapy."
He goes on further to warn that "Restrictions on gender-affirming care have also caused many people to stop or reverse their desired transitions, creating the type of involuntary detransition found in my own research." [6]
He is unambiguous. He is warning against exactly what Targownik does.
MacKinnon further states: "The Trump administration's rhetoric on detransition is dangerously myopic. We found that many people detransition not out of regret but because they feel forced to by societal factors like negative attitudes toward transgender people."[6] As we see in his quote above from his article, he documents that restrictive policies themselves create involuntary detransitions, people stop or reverse transition not because they were wrong to transition, but because social hostility made continuing unsustainable. He is saying: using detransition data to justify restrictions does not just fail logically, it creates the harm it claims to prevent.
Yet Targownik uses MacKinnon's speculative interpretation of activist-authored audit research and research found guilty of misconduct to argue for more psychotherapy, more assessment, more caution. This is effectively restricting access. She cites a researcher's citation of methodologically weak and ethically compromised research while completely omitting his explicit warnings about their misuse. She extracts numbers while leaving behind the researcher's repeated insistence that these numbers should not justify what she is advocating. This is not an innocent oversight. This is selective citation deployed to contradict the researcher's stated position while obscuring the methodological, ideological, and ethical foundations of the claims themselves.
N.B. For the record, based on a 2025 longitudinal study of 377 trans youth, the detransition rate was 2.5%.[27] For surgical regret, the data shows an even lower rate. A 2021 analysis found that in 27 studies totaling 7,928 surgery patients, the pooled regret rate was about 1%.[28]
A Rose By Any Other Name...
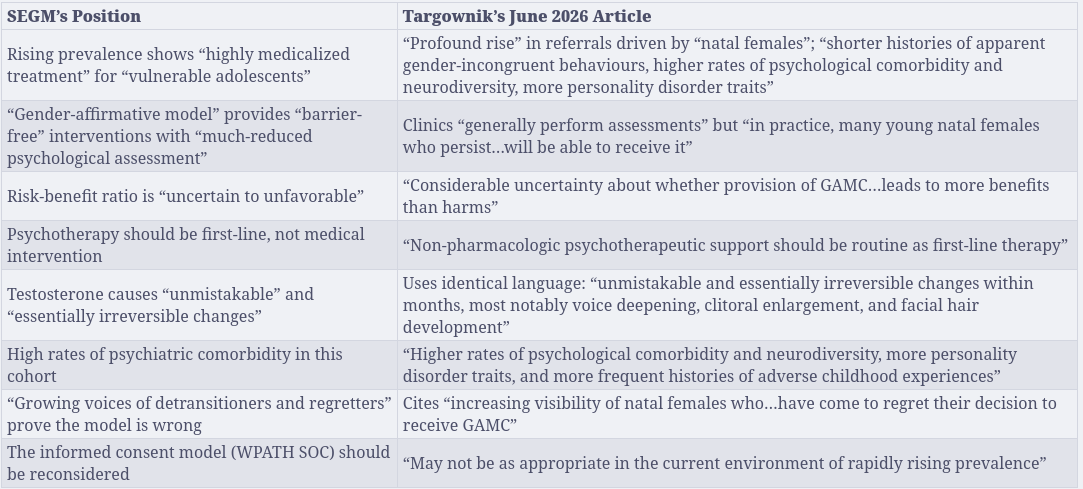
Targownik begins her article with a striking claim: "There has also been a profound rise in the number of young Canadians referred for care to Canadian gender clinics, and this rise is being driven primarily by natal females, who comprise up to 80% of young people presenting for care. Compared with earlier transition cohorts, these adolescents tend to have shorter histories of apparent gender-incongruent behaviors, higher rates of psychological comorbidity and neurodiversity, more personality disorder traits, and more frequent histories of adverse childhood experiences."[1]
She provides no citations for any of these claims. But they bear a striking resemblance and alignment to another problematic hypothesis and data set...
The Littman Trail
The 80% figure appears to come from Lisa Littman's 2018 "rapid-onset gender dysphoria" (ROGD) study. Littman surveyed 256 parents from three anti-transgender websites (4thWaveNow, Transgender Trend, Youth Trans Critical Professionals) and found that 82.8% of the youth described were assigned female at birth.[7] The accompanying claims about "shorter histories," "higher rates of psychological comorbidity and neurodiversity," "more personality disorder traits," and "more frequent histories of adverse childhood experiences" are all from Littman's ROGD framework. Targownik presents these as established clinical facts without citing Littman, without disclosing Littman's methodological failures (parent surveys from anti-trans websites, not youth data, not clinician assessments), and without acknowledging that Littman is an anti-transgender activist tied to organizations designed to restrict gender-affirming care.
ROGD is not a legitimate scientific framework. ROGD is a discredited hypothesis that has failed to be reproduced in any rigorous scientific studies. The World Professional Association for Transgender Health (WPATH) explicitly states: "The term 'Rapid Onset Gender Dysphoria (ROGD)' is not a medical entity recognized by any major professional association, nor is it listed as a subtype or classification in the Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD)." The American Psychological Association, American Psychiatric Association, and WPATH, along with 60 other medical professional organizations, have explicitly called for the elimination of ROGD from clinical settings due to lack of reputable scientific evidence.
Littman herself is embedded in anti-transgender activism. She is a principal officer of the Institute for Comprehensive Gender Dysphoria Research (ICGDR), founded in 2021 with Stella O'Malley of Genspect, an organization Yale researchers described as spreading "biased and unscientific content." Littman has contributed to anti-transgender publications and collaborated with individuals and organizations explicitly opposed to gender-affirming care for youth.
But let us be charitable. Perhaps Targownik meant to cite actual Canadian clinic data rather than Littman's parent surveys. I checked. Bauer et al. 2021, a study of transgender youth referred to Canadian clinics for gender-affirming care, found that 78.7% of youth in their sample were assigned female at birth.[8] This is close to Targownik's 80% figure. Perhaps this is what she meant to reference.
If so, she is still wrong.
What Canadian Clinics Found
Bauer et al. explicitly reject the ROGD explanation for the AFAB predominance. The researchers note: "Another reason for the shift in the AFAB/AMAB ratio is that for assigned females, pressure to rapidly conform to feminine gender norms may contribute to the urgent need for clinical services at puberty."[8] The researchers attribute the higher AFAB presentation to social pressure and gender conformity norms, not to the pathology Littman describes or that Targownik lists.
The study further found that transgender youth in Canadian clinics "were generally healthy" with presentations of "depression, anxiety, and support needs"and not the constellation of comorbidities, neurodiversity, personality disorder traits, and trauma that Targownik claims.[8] When the researchers examined actual clinical characteristics, they found health profiles consistent with youth experiencing social stress and rejection, not the pathological syndrome Littman hypothesized or Targownik characterized.
So whether Targownik is citing Littman's discredited parent surveys (without attribution), or whether she is citing Canadian clinic data (while ignoring what Canadian researchers concluded), the foundation of her argument collapses. She presents unattributed or misrepresented claims about comorbidity, neurodiversity, personality disorder traits, and trauma, claims derived from a discredited hypothesis created by an anti-transgender activist, as if they are documented features of AFAB youth seeking gender-affirming care. Canadian researchers studying the actual population found no such constellation. Littman's parent surveys, not youth data, not clinician assessments, form the basis of these claims.
What Targownik has done is take a demographic proportion (80% AFAB) and attach to it a set of psychological and developmental characteristics that are either (1) unattributed to Littman's discredited ROGD hypothesis, or (2) directly contradicted by the actual Canadian researchers who studied this population. Either way, she is laundering scientifically unsupported claims through legitimate data without proper attribution or engagement with what the legitimate data actually shows.
A Defense Worth Addressing
One might argue that Targownik's omissions reflect the practical constraints of writing for a general audience. Scientific communication for lay readers requires simplification, the argument goes, and not every citation can be exhaustively documented in a public-facing article. This defense collapses immediately when you examine Targownik's actual brand and practice. Her entire professional identity rests on precision - "the data-driven transsexual" is not a casual marketing phrase; it is her credibility marker. When precision is your brand, you do not get to claim its absence is audience-friendly simplification. The omissions are not random products of space constraints. They are systematic. They consistently excise the exact context that would undermine her argument: MacKinnon's explicit warnings and tracing the sources of his claims, the Oregon researchers' actual conclusions about access, the Bauer team's categorical rejection of ROGD.[30] Random simplification produces varied omissions across different sections. Patterned simplification produces the same strategic omission every time. This is the second kind.
N.B. It is certainly possible that Targownik possesses other yet-undisclosed sources that support her claims about comorbidity and developmental characteristics among AFAB youth seeking care. If such evidence exists, the question becomes inescapable: why does she not cite it? Why does she not share it? The silence suggests the evidence does not exist in the form she implies.
How is the Oregon Study Used?
Having made these unsubstantiated claims about the clinical characteristics of AFAB youth seeking care, claims derived from a discredited theory and directly contradicted by actual Canadian clinic data, Targownik then pivots. She writes: "A recently published study from Oregon, a US state that has made similarly progressive policy choices around GAMC, is therefore highly instructive."[1]
But here is the critical problem: the Oregon study does not address any of the clinical characteristics Targownik has just claimed. It does not measure comorbidity. It does not measure neurodiversity. It does not measure personality disorder traits. It does not measure adverse childhood experiences. It does not measure the length of gender incongruence history.
The Oregon study is a claims-based (read as: insurance claims) utilization study. It measures how many youth in Oregon's insured population received gender-affirming medical care between 2016 and 2023. That is all it measures.
Targownik is right that the Oregon study is instructive. It instructs us to draw conclusions from substantiated facts, and not from leaps. Let us see what it actually shows.
What the Researchers Concluded
The Oregon researchers actually write: "Oregon's supportive policy environment - including the 2007 Equality Act, Medicaid coverage for medically necessary transgender care since 2014, and the 2023 'shield law' (HB 2002), which prohibits insurance exclusions and requires adequate provider networks - likely contributed to greater access relative to national averages."[9]
Read the distinction carefully. The researchers conclude that the policy environment contributed to greater access relative to national averages. They are documenting that when you remove financial and structural barriers to care, more people who need care can access it. Targownik reframes this as evidence that "culture of trans acceptance and permissive policy environment may be associated with higher uptake," implying that the policy is driving unnecessary care-seeking, not enabling necessary access.
These are fundamentally different claims. One is about access. One is about excess.
The researchers further emphasize: "Insurance likely serves as a marker for intersecting structural factors rather than an independent driver of access" and that families with commercial insurance may have "advantages in navigating complex care systems, reflecting differences in socioeconomic resources, caregiver advocacy capacity, geographic access, and provider availability."[9] The study is explicit: variation in care-seeking is driven by structural access barriers and socioeconomic factors, not by a permissive cultural environment causing unnecessary medicalization.
Targownik extracts the policy finding and reinterprets it as evidence of cultural over-prescribing. She attributes causation to "culture of trans acceptance" when the researchers themselves attribute the variation to insurance access, socioeconomic resources, provider availability, and geographic access. She is speculating beyond what the evidence supports and contradicting what the researchers explicitly concluded.
Now consider the specific statistics.
The Nine-fold Increase in Context
Targownik accurately cites Oregon's raw statistic: medical gender-affirming care for AFAB youth increased nine-fold from 0.028% in 2016 to 0.25% in 2023.[9] She highlights this increase to support her implication that Oregon's permissive policy environment is driving excessive prescribing.
But here is what she does not emphasize: the nine-fold increase, while real, obscures what the study actually documents. A nine-fold increase from 0.028% to 0.25% means that in 2023, approximately one in 400 natal female adolescents in Oregon's insured population received testosterone. The study tracked 868,740 insured Oregon adolescents. Even with this nine-fold increase, the absolute number of youth receiving care remains small. The researchers' explicit conclusion is that "Medical gender-affirming care for transgender and gender-diverse adolescents is rare in Oregon."[9]
The Testosterone Comparison
Moreover, Targownik compares testosterone use in AFAB youth to estrogen use in AMAB youth, noting that testosterone use is 'four times higher than the rate seen in natal boys.' But this comparison obscures several critical confounds. First, she uses transmisic language, 'natal boys' instead of naming 'trans girls' or AMAB youth receiving estrogen. Second, AFAB youth present for care at significantly later ages (mean 15.9 years) compared to AMAB youth (mean 11.3 years), providing a longer window for testosterone accumulation.[23] Additionally, AFAB youth initiate gender-affirming care at significantly higher rates than AMAB youth (hazard ratio 2.5, 95% CI 1.8-3.3).[24] As Julia Serano notes, this disparity may reflect less stigma attached to behavioral masculinity in birth-assigned girls compared to behavioral femininity in birth-assigned boys, making it easier for AFAB youth to come out as transgender and seek medical care.[25] Research suggests this care-seeking disparity reflects broader social factors - particularly greater societal stigma toward trans women, which may deter AMAB youth from seeking care.[26] A 4x difference in hormone use rates does not indicate excessive prescribing when the demographic composition and access patterns are dramatically different. Without controlling for age at presentation and care-initiation rates, presenting this difference as evidence of, or raising concern about, over-medicalization is misleading. Particularly when doing some reading based on what we know from other studies informs us that this is, as best as we can determine, proportional and not pathological.
"Cited and Evidence Based"
What makes this worse is Targownik's claim about her own methodology. On June 22, 2026, she tweeted:
![Everything I've put in there is cited and evidence based. When there are limitations around the data, I am forward with them. When I come to my conclusions, I come by them honestly and with consideration and nuance."[10]](https://valah.blog/content/images/2026/07/image-2.png)
This is demonstrably false. Targownik does not adequately foreground or discuss the study's own stated limitations. The Gray et al. study itself notes that the data only captures insured adolescents (missing uninsured and underinsured populations), that claims data does not capture all care, and that documenting trends does not determine causation.[9] Targownik mentions none of these. She leads with the nine-fold increase without acknowledging that the study's own conclusion is that care remains rare. That is context that would appropriately scale the finding. Furthermore, she provides no additional data or context from the field of relevant studies. Instead, she uses this data point in the study out of context and in a vacuum.
Her conclusions lack the nuance she claims. She speculates beyond what the evidence supports. She reframes the researchers' finding about access as a cautionary tale about uptake. She does not acknowledge why the comparative prescribing rates actually support proportional care rather than excess. She misquotes the study's conclusions about what drives variation.
The Gatekeeping Alternatives
Psychotherapy-First: Evidence for What, Exactly?
Targownik recommends psychotherapy as first-line treatment before or in place of gender-affirming medical care. She does this while acknowledging in her own article that "there is scant evidence for psychological interventions being effective in facilitating spontaneous desistance or in improving outcomes of a subsequent medical transition."[1]
This is as interesting as it is remarkable, particularly for someone who bills themselves as "the data driven transsexual." She acknowledges the absence of evidence for psychotherapy-first approaches, then recommends them anyway. She documents the lack of evidence base, then prescribes from...hope? The belief that a child may encounter a "spontaneous dysphoria-free remission"?
This is not data or evidence driven. This is Targownik projecting their life and values on other people, and that is not medicine or science. That is ideology.
The broader research literature supports this skepticism. The American Psychological Association notes that "attempts to change sexual orientation or gender identity are some of the most damaging practices in the history of mental health." Studies consistently show that talk therapy does not change gender identity. When psychotherapy is beneficial, it is when it supports a person's authentic identity, including gender transition, not when it attempts to prevent or discourage it.[13,14] The evidence is clear: psychotherapy used to suppress gender identity harms people. Psychotherapy used to support gender identity helps people.
What does change with psychotherapy? Distress decreases when a person is supported in their gender identity. Distress increases when they are encouraged to suppress it. This is not ambiguous. This is documented.
Targownik is recommending an intervention that the evidence base does not support, acknowledges the lack of evidentiary support, and which research suggests may be harmful when used to delay or discourage transition. This is not evidence-based or data-driven medicine. This is ideological-based medicine in a white coat.
In a more charitable read, Targownik could be expressing the idea that psychotherapy-first is not an attempt to change one's gender identity, which would appear to align with her inferred values, but as a means to "wait and see" while exploring where the dysphoria comes from and an attempt to measure how "insistent, consistent, and persistent" it is.
This is a more defensible framing. But it still fails for three reasons.
The "Wait and See" Defense
First, Targownik herself has already foreclosed this defense. She acknowledged that "there is scant evidence for psychological interventions being effective in facilitating spontaneous desistance." If the goal is to "wait and see" whether dysphoria resolves, and the evidence shows psychotherapy does not facilitate that resolution, then what exactly is the youth waiting for? The exploration has no defined endpoint, no measurable threshold for completion, and no evidence base indicating it achieves its stated purpose. It is an indefinite delay dressed as assessment.
Second, "wait and see" is not a neutral act. The evidence is clear that delays in gender-affirming care are not benign. Tordoff et al. found that youth who did not initiate hormone treatment within the first three to six months of care experienced a two- to three-fold increase in depression and suicidality.[20] Turban et al. found that transgender adults who accessed hormone treatment during adolescence had significantly better mental health outcomes than those who waited until adulthood.[21] "Waiting" has a documented cost. It is not the absence of intervention, it is an active decision to withhold an intervention with documented benefits while a youth's mental health deteriorates. The charitable framing assumes the delay is harmless. The evidence says it is not.
Third, "insistent, consistent, and persistent" is itself a general rule of thumb for parents to observe in their children starting at an early age. It is not supposed to be used as a gatekeeping framework, and is not a clinical framework. To use it as such requires youth to perform their suffering over an extended period, to demonstrate that their dysphoria is sufficiently severe, sufficiently enduring, and sufficiently unwavering to satisfy an evaluator's standard of legitimacy. But the Bauer et al. study of Canadian clinic populations found youth were "generally healthy" with "depression, anxiety, and support needs."[8] Not a population requiring extended diagnostic surveillance to rule out pathology. The framework assumes that dysphoria is suspect until proven otherwise, that the burden of proof falls on the youth, and that the default position is restriction rather than care. It inverts the standard: instead of providing treatment and monitoring outcomes, it withholds treatment while demanding proof that the treatment is warranted, "just to be sure." Proof that, by Targownik's own admission, psychotherapy cannot produce.
The "wait and see" defense replaces one problem with another. It concedes that psychotherapy is not conversion therapy, but it preserves the same functional outcome: delayed access, prolonged distress, and a gauntlet of proof before care. Calling it "exploration" rather than "gatekeeping" does not change what it does. A door that is locked while someone decides whether you deserve to walk through it is still a locked door, regardless of how thoughtfully the lock is considered.
Support vs. Gatekeeping
The strongest defense of psychotherapy-first approaches is that they function not as a replacement for medical care but as a genuine concurrent support, that exploration and assessment represent good clinical practice, not gatekeeping. This distinction matters. It matters enormously. If psychotherapy accompanies transition and supports a young person's authentic identity, it serves them. If psychotherapy precedes and delays transition pending uncertain outcomes and unspecified thresholds of proof, it restricts access. These are different architectures producing different outcomes.
Targownik's framing is unambiguous about which architecture she is advocating. She recommends psychotherapy as "first-line therapy," requires "long-standing objective evidence" of dysphoria before medical intervention, and suggests deferral wherever it is "possible to tolerate." These are sequential gates, not concurrent supports. The youth must pass through psychotherapy first, demonstrate sufficient evidence of persistent dysphoria, and prove they can endure waiting, then perhaps medical care follows. This is not "psychotherapy alongside transition." This is "psychotherapy instead of transition, unless and until you meet undefined criteria of severity and persistence and proof." The architecture is sequential restriction, not concurrent support.
Targownik further recommends that "decisions around the initiation of testosterone...be deferred" and suggests that "continuous oral contraceptives or progestin-based methods" can address dysphoria-related menstruation, allowing testosterone to be delayed or avoided entirely.[1]
This claim requires examination of what the evidence actually says, and more importantly, what it reveals about the logic underneath.
Partial Relief as Gatekeeping
The contraception study Targownik cites concludes: "TGD AYA [Transgender Adolescent/Young Adult] patients may seek contraception care that is discrete, avoids estrogen, helps alleviate gender dysphoria, and potentially leads to amenorrhea."[15] And further: "There continues to be a need to assess contraception use and preferences in TGD adolescent and young adults."[15]
What this study actually documents is that transgender youth seek contraceptive methods that suppress menstruation. That is not the same as claiming that menstrual suppression alone addresses gender dysphoria or makes testosterone unnecessary.
The distinction matters clinically and ethically. Targownik conflates two separate problems:
- Dysphoria from menstruation specifically
- Systemic gender dysphoria from sex characteristics across the body
Contraceptive-induced amenorrhea addresses the first. Testosterone addresses the second, plus the constellation of other concerns — voice, facial hair, body fat distribution, muscle development, etc — while menstrual suppression alone produces none of these outcomes for systemic dysphoria. The research on what addresses the second is unambiguous: "decreased depression, anxiety, suicidality, self-harm, gender dysphoria, and body dissatisfaction, as well as increased quality of life and life satisfaction."[20,21] These outcomes are associated with gender-affirming hormone therapy, testosterone in transmasculine individuals, not with menstrual suppression through contraception alone.
At best, for some youth, contraception may help manage their dysphoria regarding menstruation specifically — which the research shows is indeed valued. But using that as justification for deferring testosterone does not follow logically. You are treating one specific part of dysphoria while withholding treatment for systemic dysphoria. The logic is not medical. It is gatekeeping.
Offering contraception-induced amenorrhea as a substitute for testosterone is, at best, partial relief—like giving 50 milliliters of water to a person dying of thirst in a desert. Just enough to keep them alive a little longer, dangling the full canteen just out of reach. At worst, it is withholding care as an interrogation means, dressed up as compassionate concern.
Targownik is performing a sleight of hand. She takes a study about preferences for menstrual management, what youth want from contraception, and extracts from it permission to defer access to testosterone. But the study documents no evidence that amenorrhea-inducing contraception addresses systemic gender dysphoria or makes testosterone unnecessary. It documents only that youth want menstrual suppression and that research gaps remain about how to provide it safely and effectively.
What Lies Beneath the Arguments?
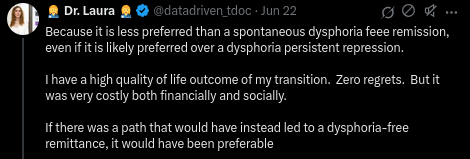
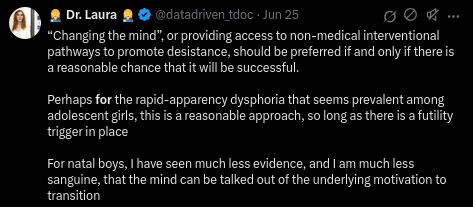
When pressed about her gatekeeping stance on social media, Targownik revealed her underlying framework in a June 2026 Twitter exchange. She explained her position on "rapid-apparency dysphoria" (ROGD language, softened):
This statement begs the question it pretends to answer. She assumes AFAB rapid-onset dysphoria is less real or more reversible ("talked out of") than AMAB dysphoria, then uses that assumption to justify psychotherapy-first. But she provides no evidence that AFAB dysphoria is reversible. She provides no evidence that psychotherapy can successfully discourage or resolve it. She assumes the premise ("rapid-onset means less real") and calls the conclusion evidence-based ("therefore psychotherapy-first is reasonable"). This is putting aside the fact that there is not credible evidence that "rapid-onset dysphoria" is even a real phenomena, or just a mis-perception attributed to a much more plausible and likely circumstance: we discovered a lot more stars and planets once we discovered telescopes, and that when we stopped punishing people for being left-handed, we 'suddenly' had a surge in left-handed people in the world. Occam's razor applies.
The statement also reveals her underlying hierarchy: AMAB dysphoria (early-onset, persistent) is real and immutable. AFAB dysphoria (recent-onset, rapid) is suspect and reversible. Psychotherapy-first makes sense for the "suspect" dysphoria. Restriction makes sense for the "suspect" population.
Whose Dysphoria Counts?
Targownik identifies publicly as a transmedicalist.
Transmedicalism is a hierarchical framework that ranks whose gender dysphoria "counts" as legitimate ("really trans") based on specific criteria: onset trajectory, duration, severity, and consistency of presentation (see: transmedicalism.info - in case of a 404 error, simply refresh the browser).
It is a fringe stance within the trans community. Outside it, this is simply pathologization of a minority's care and the resultant paternalistic gatekeeping of said minority.
Under transmedicalism, some dysphoria is "real" and deserves medical response. Other dysphoria is suspect, reversible, or insufficiently severe (the degree and stance varies by transmedicalists, they are not a monolith). This framework explains Targownik's differential treatment of AFAB and AMAB dysphoria and "rapid-onset" versus "early-onset." It explains why she assumes AMAB early-onset dysphoria is "immutable" while AFAB rapid-onset dysphoria is "reversible." It explains the gatekeeping logic: certain youth must prove their dysphoria meets the threshold of legitimacy before access to care.
This is not evidence-based medicine. It is an ideological stance, where in the ranking dysphoria by its trajectory and assigning care accordingly determines who is "really trans" or "one of the good ones that will have positive results/outcome." Gatekeeping is not incidental to transmedicalism - it is the framework's entire function. To rank dysphoria by legitimacy, you must have gatekeepers deciding which dysphoria counts. The ideology requires someone to determine who is 'really trans' or 'one of the good ones.' The effect is gatekeeping wrapped in psychological and medical pathologization, and it is exactly the kind of hierarchy that leads to differential treatment based on nothing more substantial than timing, body, and clinician vibes.
The Architecture of Restriction
Targownik's article exhibits several characteristic logical and/or rhetorical moves that deserve further examination:
Appeal to Authority: White Coat Legitimacy sans Expertise
The Fallacy: Targownik invokes her credentials as a physician and epidemiologist to speak with authority on gender medicine, despite having no clinical work with trans youth, no published research in gender medicine, and no formal training in gender-affirming care. Her credentials speak only to training in gastroenterology and disease utilization patterns (epidemiology). Yet a reader encountering the article sees "MD" and "epidemiologist" and grants authority on gender medicine that her actual credentials do not support. Epidemiology is the study of disease patterns and etiology, and though it should go without saying, but gender identity is not a disease. The credentials become a stand-in for expertise they do not represent. It provides rhetorical cover that obscures the gap between her formal training and the unrelated domain she is addressing.
Absence of Evidence as Evidence of Absence: A Layered Set of Fallacies
Argument from ignorance layered with asymmetrical burden of proof, essentially dismissing valid data while requiring perfect data.
The Fallacy: Targownik documents the absence of evidence that psychotherapy works for this population, then uses that absence as justification to recommend it first-line. She treats lack of evidence as evidence of safety ("likely minimal adverse effects"). Simultaneously, she treats uncertainty about long-term testosterone outcomes as justification for restricting access to an intervention that does have evidence of benefit. The evidentiary standard is asymmetrical: lack of evidence for X becomes a reason to use X, while good evidence for Y becomes a reason to defer Y. She also dismisses existing long-term data as "low quality" or "low certainty" while simultaneously using the absence of different long-term data as justification for gatekeeping. "Low quality" does not mean "invalid," "suspect," or "speculative," it is valid evidence that should be weighed, not dismissed. She demands perfect/high certainty before permitting access while accepting uncertainty as sufficient reason to restrict it. This is not evidence-based medicine. It is ideology disguised as caution, wrapped in the language of care.
Soft Restriction as Measured Caution: A Rhetorical Strategy/Fallacy
Could otherwise be considered a form of doublespeak or linguistic obfuscation.
The Fallacy: Targownik frames her position as "support" for access "in the right circumstances" while simultaneously recommending psychotherapy-first, undefined criteria for access, and deferral wherever "manageable" to delay. But psychotherapy-first is not support for access, it is prioritizing a different intervention before access to the requested one. "Where it can be tolerated" is not clinical guidance, it is discretionary threshold-setting based on pain tolerance and clinician judgment. She is architecting restriction while using the language of care and measured caution. The soft language obscures the hard gatekeeping. A reader sees "I still believe access can help" and misses "I am recommending you wait, prove yourself, jump through these narrowing gates."
Selective Evidence: Cherry Picking with Confirmation Bias
The Fallacy: Targownik cites two systematic reviews to support her claim that "considerable uncertainty" exists. However, both reviews were funded by the Society for Evidence-Based Gender Medicine (SEGM), an organization explicitly dedicated to restricting gender-affirming care and has been classified as a hate group by the Southern Poverty Law Center. All authors of both papers have a long standing affiliation with SEGM.
More importantly, Targownik presents these two reviews as representative of "the available literature" without acknowledging that far more comprehensive, long-term, and consistent evidence to the contrary exists, evidence showing that gender-affirming care improves mental health outcomes and reduces suicidality in transgender youth. She omits any citation to systematic reviews or meta-analyses demonstrating these benefits. She selects conflicted reviews that align with her gatekeeping position while omitting non-conflicted evidence that contradicts it. This is not literature synthesis, and it is not her being data-driven, transparent, and reasoned, or in her own words:
Furthermore, with various claims throughout her article, Targownik focuses extensively on detransition rates and potential long-term harms of testosterone while downplaying the documented harms of delay, denial, and gatekeeping itself. She presents detransition rates without context: external pressures, discrimination, lack of family support, and restriction-induced detransition (MacKinnon's own finding). The evidence she selects builds a narrow narrative: "testosterone can be harmful" while omitting the equally valid narrative: "restriction can be harmful" while simultaneously omitting the known benefits. Selective evidence is not evidence-based analysis, selective data points is not being data-driven.
It is narrative-building in service of a predetermined conclusion.
Begging the Question: Assuming the Premise She Is Trying to Prove
Targownik: "Which raises an obvious question: given this uncertainty about the risks and benefits of long-term testosterone exposure in dysphoric natal females, how comfortable are we in Canada in continuing a set of policies and clinical norms that may be contributing to this significant rise in use?"[1]
The Fallacy: She presents rising rates of testosterone use as evidence of a problem requiring policy change. But she never establishes that rising rates indicate inappropriate care. She assumes the premise ("rising rates are concerning") and frames the conclusion as inevitable ("therefore we should change policy"). A more parsimonious explanation: rising rates reflect improved access to diagnosis and care for a population previously underdiagnosed and undertreated. Appropriate care naturally produces higher rates when previously denied populations gain access. She does not prove rising rates indicate overmedicalizing. She assumes it.
Undefined Terms/Vagueness: Technical Language as Gatekeeping Mechanism
Targownik: "Most importantly, testosterone-based GAMC should be considered only when there is an established long-standing objective evidence of dysphoria, sustained integration in the gender role associated with the target sex, or if there is evidence of clinically meaningful worsening of mental health which can be ascribed to ongoing dysphoria despite psychological interventions."[1]
The Fallacy: She provides no definitions for "long-standing" (1 year? 3 years? 5 years? Before puberty onset?), "objective evidence" (self-report? behavioral observation? what threshold?), or "established" (by whom? what standard?). She has written gatekeeping criteria in language that sounds clinically rigorous while remaining utterly subjective. A clinician can cite "insufficient objective evidence" to deny care. A different clinician can accept the same presentation as "established long-standing objective evidence." The criteria are not objective. They are subjective and a discretionary power dressed in technical language. That is not evidence-based medicine. That is the architecture of restriction.
Finally, what is notable is that all of these fallacies and rhetorical moves are wrapped in measured, cited, and careful language. They are not crude or obvious. They are respectable, and the form obscures the content. A reader encountering this article sees what appears to be evidence-based analysis from a credentialed, knowledgeable person who happens to have the additional credibility of the lived experience of a trans woman, and not the logical or rhetorical fallacies. That is the power of the presentation, and why it is dangerous without critical thought and/or prior knowledge of the field.
The Past is Prologue
A Pattern Emerges
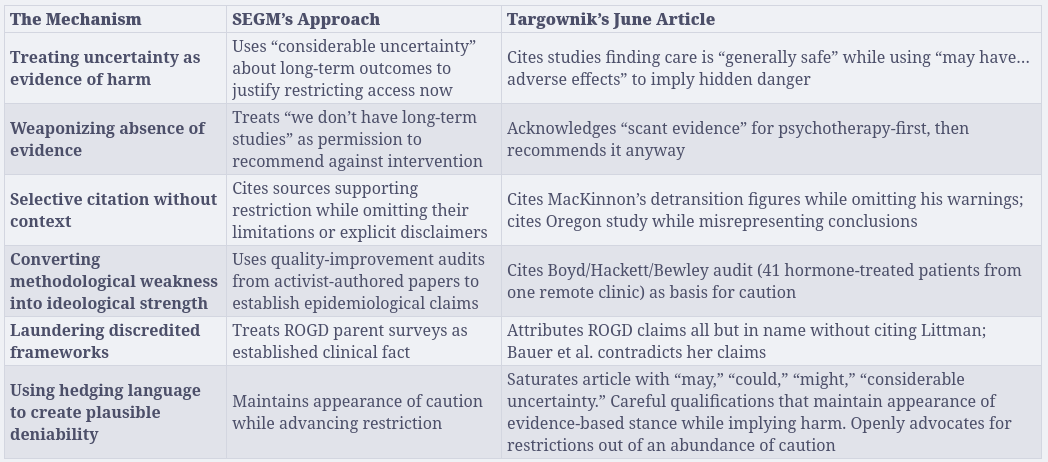
The June article deploys three major and specific mechanisms, each identifiable, each repeated. They are not accidents of style or tone. They are architectural.
First: Assumption Without Verification. Claims about AFAB youth are presented without citation: "shorter histories of apparent gender-incongruent behaviours, higher rates of psychological comorbidity and neurodiversity, more personality disorder traits, and more frequent histories of adverse childhood experiences." When sources can be traced, they lead to discredited frameworks or are misrepresented. The assumption precedes the evidence.
Second: Representing Unreliable Information as Fact. Littman's ROGD framework is laundered through unattributed references. MacKinnon is cited without disclosing his explicit warnings against Targownik's conclusions or the basis of his numbers and their problematic origin. The Oregon study is cited while misrepresenting the researchers' conclusions. Hedged language ("may have," "could," "might") is deployed as evidence-based caution while speculative risks justify gatekeeping. The form obscures the function.
Third: Selective Citation and Omitted Context. MacKinnon's detransition figures are quoted while his warnings about misuse are omitted. Studies concluding care is "generally safe" are cited while using conditional language that implies harm. The Oregon researchers' attribution of variation to structural barriers is ignored in favor of cultural over-medicalization or being over-permissive. She demonstrated in April that she understood these mechanisms perfectly. In June, she deployed them anyway.[31] In June, she omits them strategically.
These three mechanisms are not unique to June. They often appear together, sometimes even in the same sequence, in her Twitter exchanges on ROGD and gatekeeping, and throughout many of her social media, blog, and podcast content.
A Twitter Thread Reveals
As just one example to highlight, in January of this year (2026) Targownik deployed these three mechanisms in a Twitter exchange on ROGD/"Social Contagion" and gatekeeping. The exchange is instructive because it captures the pattern under pressure and what happens when she is challenged in real-time to substantiate her claims.
Assumption Without Verification (Opening Position):
Targownik opened with a declarative claim (paraphrased for simplicity): "We need to accept that this is a thing that happened — Social media and other cultural elements likely induced gender dysphoria in some adolescents who might not have otherwise experienced it."
No citation. No data. No caveat. The claim is presented as something that must be accepted - a fait accompli requiring agreement, not evidence.
Representing Unreliable Information as Fact (Under Pressure):
When challenged to provide empirical support, she did not cite studies. Instead, she shifted the framing: first it is the hedging of "this is emerging data" and when pressed to show that data, it becomes "i am not claiming it is a proven theory." She reframed from "we need to accept this happened" to "it's the most compelling active hypothesis."
But the reframing only occurred after being pressed. The initial move, present speculation as established fact, remained unchanged.
She then used epidemiological authority to legitimize the hypothesis, to paraphrase the thread so far: "...as an epidemiologist... I see [social contagion] as the most compelling active hypothesis," framing her professional credentials as evidence for the claim itself.
But social contagion is not an active hypothesis, it is a thoroughly discredited and debunked hypothesis. [29]
Furthermore, this particular tweet commits a category error wrapped in her appeal to authority (her credentials). Targownik frames the rise in trans identification through epidemiological language, 'emergent exposure,' 'case-ascertainment,' invoking professional authority to suggest that social and cultural factors are causing trans identity like a virus causes infection, or that it is spreading in a similar fashion - but the correlate to her example in this thread is social contagion. But epidemiology studies pathological conditions, not one's identity. Applying outbreak logic to one's identity requires the unstated premise that trans identity is itself pathological. Moreover, she acknowledges case-ascertainment effects (improved visibility due to reduced gatekeeping) as a possibility, then dismisses it in favor of 'emergent exposure' without evidence. This isn't epidemiology. It's transmedicalism dressed in scientific language.
Selective Citation and Omitted Context (Substantive Evasion):
When people cited studies contradicting her position, she did not engage with what those studies said. She dismissed them categorically: "people have posted well-intended but flawed studies that do not disprove" her hypothesis.
She did not identify what made them flawed. She did not address their actual findings. She deflected the substantive challenge by questioning the methodology of the challengers rather than engaging with the evidence.
The Mechanism Revealed:
What the Twitter exchange demonstrates is the three mechanisms in sequence and under pressure:
- Make an assumption or belief claim and present it as fact
- When challenged, hedge the claim while using authority to legitimize it
- When asked for evidence, or evidence contradicts you, dismiss the evidence without substantive engagement
This is not how evidence-based analysis works. It is how narrative management works.
The Pattern in History: March 2020
But this is not new. Six years before June 2026, under professional scrutiny, Targownik deployed the exact same three mechanisms.
In March 2020, the College of Physicians and Surgeons of Manitoba ("Canada's provincial medical licensing body") issued a formal censure of Dr. Laura Targownik (#IC4235). The pattern they documented was precise: she had represented unreliable information as fact, made assumptions without verifying them, when concerns were raised, did not engage substantively with those concerns and finally, had "inappropriately referenced information that had come to her attention as a physician leader."[17]
The censure stated explicitly: "It is aggravating that Dr. Targownik did so based on unreliable information that she represented as fact."[17]
Specifically, the Committee found that Dr. Targownik had:
- Made assumptions about a patient's personal situation without verifying them (financial circumstances, immigration status, knowledge-state)[17]
- Failed to verify basic facts before making public statements[17]
- Inappropriately referenced information obtained through her position as physician-leader[17]
- Been "not aware of the facts" while presenting her concerns as established fact in a national forum to 7,800 physicians[17]
- Not discussed concerns directly with the subject of her critique before publicizing them[17]
The Committee's conclusion was direct: "she should have made an effort to discuss the matter with him first, or, in the alternative, limited the communications about her concerns to bringing them forward to the appropriate authority."[17]
Instead, she published unverified claims in a national forum with widespread professional visibility, damaging a colleague's reputation based on assumptions she had not verified yet presented as fact.
The Architecture is Habitual
The three mechanisms are not confined to one article or one Twitter thread. They form a pattern documented under professional scrutiny in 2020, deployed in real-time on social media and throughout much of her content, and reflected with sophistication and intent in her June 2026 article.
What makes this pattern significant is not that it happened once. It is that she knows what these mechanisms are, how they function, and how they undermine substantive analysis. Her April article demonstrates this knowledge explicitly.[31] Her past disciplinary record shows she has been held accountable for this in the past. Next we will examine how, within weeks, she deployed them anyway.
The Machinery
In April 2026, Targownik documented with meticulous precision how SEGM weaponizes research in an article titled "What the Finnish Register Study Can and Cannot Tell Us About Mental Health in Gender-Dysphoric Youth." on her Substack blog.[31] She identified their methods with granular specificity: how uncertainty about outcomes gets converted into justification for restriction, how methodological limitations get treated as evidence of harm, how silence on a topic gets converted into consensus against an intervention.
Her April analysis demonstrated that she understands these mechanisms completely. She can identify them. She can articulate why they are intellectually dishonest.[31]
Yet what is instructive about her April analysis itself is that even while surgically precise about SEGM's methods, it remains curiously charitable about their motivations. She acknowledges their work "had to anticipate that results...would be overgeneralized," even suggesting the risk of misuse was "quietly welcomed."[31] But then she softens, attributing the methodological choices to budget constraints and data reuse rather than to deliberate design. She does not interrogate why they selected crude outcome measures when richer ones existed in the dataset, or why the decision architecture consistently skewed toward one conclusion.
This matters because Targownik operates from within the same epistemological framework as those she critiques. She can identify SEGM's data misuse while remaining generous about their intent because she shares their underlying assumption: that caution about medical transition is defensible even when the evidence does not require it. She critiques their tactics while accepting their premises. Her April analysis, rigorous as it is, remains bounded by a gatekeeping logic she does not interrogate. She does not ask why transition faces higher evidentiary demands than other medical interventions, or why "insufficient evidence" consistently translates to "restrict access" rather than "conduct better research with protected access."[31]
When someone can identify a mechanism so precisely, explain its dishonesty so clearly, and then deploy it themselves, the question shifts. It is no longer whether they understand the machinery. They clearly do. The question becomes whether the machinery itself has become inseparable from their thinking - whether understanding it and operating it have become the same act.
On April 24, she was explicit:
This is an accurate description of confirmation bias in research evaluation. It is also precisely what she does in her June article. She promotes low-quality research without criticism when it aligns with her prior (that affirming care needs gatekeeping). She picks apart higher-quality research when it contradicts her prior (by dismissing the researchers' explanations as ideologically motivated).
Not in broad strokes. Not in general principle. But mechanism by mechanism, almost point for point.
The Playbooks Side by Side
This is not coincidence. Coincidence requires independent arrival at the same position. This does not appear to be coincidence. This is application of a documented playbook by someone who has publicly explained exactly how the playbook functions and why it is dishonest.
The Mechanisms in Practice
The Cardiovascular Example
The study Targownik cites on cardiovascular effects concludes: "The available evidence on cardiovascular mortality associated with testosterone therapy...the absence of cardiovascular deaths in short-term randomized trials does not allow inference regarding long term cardiovascular safety, highlighting the need for adequately powered studies with extended follow-up."[18]
What the study actually says: No cardiovascular deaths were observed in short-term trials. We cannot use that short-term data to conclude anything about long-term safety. We need better long-term research.
What Targownik claims: Testosterone "may also have clinically relevant adverse effects on markers of cardiovascular...health."[1]
She has converted "we observed no deaths but need more research" into "there are likely adverse effects." This is the precise move she documented SEGM making in April.[31] She identified it as intellectually dishonest. She is now deploying it.
The Liver Study Example
The study on liver safety concludes with absolute clarity: "Current studies indicate that recommended GAHT formulations are generally safe, with few hepatic side-effects" and most directly, "Based on the best evidence currently available, modern GAHT is generally safe from a hepatology perspective when used according to guidelines."[16]
What the study actually says: GAHT is generally safe. We have identified knowledge gaps we should study further.
What Targownik claims: It "may also have clinically relevant adverse effects on...markers of...liver health."[1]
She is performing the exact maneuver she documented SEGM doing in April: treating "we need better research" as "evidence of harm."[31] The study says this is safe. She cites it to suggest it might not be. She uses conditional language to create plausible deniability while implying risk.
The Benjamin Ryan Connection
When Targownik hosted Benjamin Ryan in a February 2026 podcast, she concluded by describing him as "an honest broker" who "takes an honest look at the data."[22] What does an "honest look at the data" mean in practice?
Taking an "honest look at data" means engaging with how the researchers who collected it interpret their own findings. It means substantively addressing their explanations if you disagree. When Ryan examines the Oregon study, he accepts the raw numbers but dismisses the authors' evidence-based explanations: that variation reflects "guideline-concordant assessment," "variable timing of gender identity development," and "barriers or delays in accessing care." His dismissal is cursory: "I cannot see how they can know any of this based on simply looking at these data."[19]
He then substitutes a speculative ideological explanation: that Oregon's progressive culture explains the variation. This is not supported by the data. It is not evidence-based. It is an assumption that serves his predetermined conclusion.
This is not an honest look at data. It is accepting data while rejecting methodology and replacing it with ideology.
Yet Targownik, who would document these same mechanisms as dishonest gatekeeping tactics just two months later in April, endorsed Ryan's work as "honest" and described him as taking "an honest look at the data." She even adopted his framing of the Fox Varian case as her opening narrative, then performed critical engagement by pushing back on specific data points (puberty blocker continuation rates) while leaving his core premises untouched: that ROGD (social contagion) is a clinical phenomenon, that affirming care is "whatever you say goes," and that SEGM's concerns, while aggressively pursued, identified real problems.
This is a pattern: critical scrutiny of details, absorption of premises. She receives credit for engaging carefully while the foundational architecture passes through unchecked.
The question becomes unavoidable: Does she genuinely believe Ryan is an honest broker? Or does she recognize that his methodology mirrors SEGM's documented gatekeeping apparatus, and she is credentialing him anyway because his conclusions align with her own?
Either answer is damaging. The first suggests she cannot recognize the mechanism she spent April documenting.[31] The second suggests she recognizes it and endorses it when its convenient for her own narrative.
Validators of a feather...
The National Post article that includes Targownik is not neutral journalism documenting multiple medical perspectives. It is an outlet with a documented conservative editorial stance, AllSides rates it as "Lean Right," systematically publishing content skeptical of gender-affirming care: "Doctors and parents need to rethink 'gender-affirming care' for children," "Groundswell against gender-affirming care becoming too loud to ignore," and "Take a cautious approach to gender-affirming treatments for minors."[12] The National Post's coverage pattern is systematic: it emphasizes polling data showing public skepticism, platforms experts expressing caution, and frames the issue through the lens of "vulnerable youth" needing protection.
In this context, the National Post article strategically positions medical professionals as validators of skepticism toward gender-affirming care. And the doctors it interviews? Three clinicians expressing caution: Dr. Gordon Guyatt (affiliated with SEGM and its restrictive positions), Dr. Karine Khachatchourian (who says she would challenge "medicalizing the majority" while maintaining "I strongly believe in this care"), and Dr. Laura Targownik (who advances most SEGM talking points wholesale).
The National Post frames these as independent experts reaching similar conclusions about the need for caution. What they actually represent is three different expressions of the same gatekeeping agenda, dressed in different rhetorical framings, offering three different validators to choose from: the experienced researcher and scientist; the "I used to believe in this" clinician turned skeptic; the trans validator—"I am trans and even I think this is concerning."
All three recommend the same functional outcome: fewer youth accessing care, delayed access, and more gatekeeping barriers.
The critical insight is this: "more rigorous assessment" is gatekeeping. When you add psychotherapy requirements, extend assessment timelines, require "long-standing objective evidence" of dysphoria, and defer access pending this "rigor," you have restricted access. You have narrowed the gates and simply called it something else. Khachatchourian's "more rigorous care" and Targownik's "evidence-based caution" and Guyatt's established SEGM positions are functionally identical: they all result in fewer youth receiving timely care.
This matters because Targownik presents herself as an independent voice: pragmatic, data-driven, guided by evidence rather than ideology. Yet her documented alignment with SEGM-affiliated researchers, her selective engagement with figures like Ryan, her adoption of many of SEGM's talking points wholesale, and her self-identification as a transmedicalist reveals a more constrained and ideological position.
It is not a neutral position or ideology. It is the framework that transforms gatekeeping from deviation into principle, which is precisely what makes it so difficult to challenge from within the community.
The Harm
So where does that leave us?
Targownik has given us the answer herself. In April 2026, she documented with meticulous precision how SEGM weaponizes uncertainty, how methodological weakness becomes ideological strength, how the language of caution obscures the machinery of gatekeeping. She identified the mechanisms. She articulated their dishonesty. She explained exactly how they work.[31]
Then she uses them. Not in broad strokes. Not in general principle. But mechanism by mechanism, almost point for point. The same conversion of absence of evidence into permission to restrict. The same selective citation stripped of context. The same hedging language that maintains plausible deniability while implying harm. The same laundering of discredited frameworks through careful attribution games. She has become precisely what she diagnosed.
This would be simply ironic if the target were her intellectual consistency. But the target is not abstract. The target is real youth experiencing genuine distress. About 8500 that we know of in Oregon. Thousands in Canada. Youth whose only crime is seeking help from a medical system increasingly gatekept not by evidence but by the carefully constructed respectability politics of people who understand the machinery well enough to operate it.
What makes Targownik's position particularly effective, and particularly dangerous, is not accidental. She stands behind credentials and a white coat. She speaks both from within the medical establishment and from a trans identity. She can articulate "legitimate medical concern" in language that, word for word, would be transmisic gatekeeping if spoken by a cisgender physician. But because she speaks from the position of both medical expertise and community membership simultaneously, those same mechanisms become legible as rigor rather than restriction. The machinery is harder to see when it is operated by someone the community has reason to believe should be on their side.
The machinery works because it is dressed in the right language, deployed by the right credentials, embedded in the right professional networks, and delivered by someone the community has trained itself to trust - one of their own. Targownik has become fluent in that language. At what point does operating the machinery you have publicly exposed become indistinguishable from the machinery itself?
What Honest Scholarship Actually Requires
This analysis is not to establish that gender-affirming care requires no scrutiny. It does. Every medical intervention warrants rigorous evaluation, honest assessment of outcomes, and willingness to revise protocols as evidence accumulates. The question is not whether scrutiny is appropriate. The question is how that scrutiny is conducted.
Honest scholarship on pediatric gender medicine would:
- Cite sources with their full context, including limitations the researchers themselves identified
- Distinguish between absence of evidence and evidence of absence—between "we don't have long-term data" and "we have evidence of harm"
- Represent the conclusions researchers actually reached, rather than reframing them to serve a predetermined position
- Acknowledge when cited researchers explicitly warn against the specific use being made of their work
- Disclose methodological weaknesses in sources relied upon—including author affiliations, ethical findings, and documented ideological positioning
- Maintain consistency between the standards applied to evidence supporting one's position and the standards applied to evidence challenging it
- Recommend interventions only when the evidence base supports them, or clearly label recommendations as values-based rather than evidence-based
- Avoid hedging language that maintains plausible deniability while implying conclusions the evidence does not support
None of these are unreasonable standards. They are not partisan. They are not advocacy-driven. They are the baseline standards of intellectual integrity. They are the standards Targownik herself articulated in April 2026 when she diagnosed SEGM's dishonesty. They are the standards any clinician presenting themselves as "data-driven" should meet without question. They are the standards that protect youth—whether those youth need access to gender-affirming care or protection from premature or inappropriate intervention—because honest evidence is what enables clinicians, families, and young people to make genuinely informed decisions rather than decisions shaped by carefully constructed narratives.
What makes gatekeeping dangerous is not that it is crude or obvious. What makes it dangerous is that gatekeeping disguised as caution does not protect youth. It simply makes the harm invisible by renaming it. And when that gatekeeping is performed by someone with credentials, community standing, and the ability to quote-mine evidence with precision, it becomes nearly impossible for families and young people to recognize what is actually happening until they are already caught in the machinery.
In Closing...
While finishing this article I found myself conflicted. Dr. Laura Targownik is very much likely operating from her sincerely held beliefs and her position is one she has probably arrived to through her own means of contextualizing and rationalizing her own life experiences of being trans and transitioning coupled to her formal education and training from within the values and principles she holds, portrayed through her own socio-political lens from which she views herself and the world around her. This undoubtedly leads her to arrive at the conclusions she does. Whether this is due to her political and ideological alignment, out of her best educated analysis, or due to greater ambitions that result from this alignment, I can't say, and I won't begin to speculate.
What we can say is this: the striking similarity between what she critiques in April and what she writes in June, combined with her own discussions and rationalizations witnessed across social media platforms in real-time, confirms beyond question that a confirmation bias is self-evident and aligns with the likes of SEGM and various researchers, journalists, and platforms with a particular political and ideological stance.
Was this piece pointed at the wrong person, and in the wrong direction? Was it too critical against one of our own, and would it better serve our rainbow community if I left it on a shelf, unpublished?
Then the day before I finished the polish on this article, Dr. Rachel Saunders published a great one on Medium entitled "Dear LGBTQI+ community, we need to talk about evidence" that perfectly captures why we are having this conversation. She made a simple observation: articles claiming to be evidence-based must actually have and show evidence. They must link to their sources. They must show their work. As Saunders puts it, "When I write from an evidence-based position I link directly to my sources, allowing scrutiny of the data and constructive deconstruction of my arguments. This is essential to allow robust critique."[32]
But here is where it gets interesting. Saunders is equally clear about what happens when someone refuses to do that. When they claim authority without showing their work. When they cite studies they have not actually read, or read selectively, or misrepresented. When they build an entire argument on foundations they will not let you inspect. Saunders has a word for that. She calls it propaganda.[32]
And propaganda, she notes, "potentially causes much more harm to our communities than they realise."[32]
Now, Targownik's June analysis does link to some of the studies she cites, others we have to dig in order to find them. She does not acknowledge the limitations of her sources, the problematic affiliations of their authors, or the breadth of existing data that contradicts her conclusions.. It does not show how she arrived at conclusions the evidence does not support. It presents selective narratives as fact while hiding the apparatus that selected them, wrapped in her credentials as authority, and her identity as a shield.
To summarize in the words of one "data-driven transsexual," "They have a preferred outcome, and they selectively promote narratives and evidence that seek to eliminate one particular modality of care for gender-distressed youth."[33]
That is precisely what happened here. And in the closing words of Dr. Saunders:
"It is not too much to ask for those claiming authority to show their working out, to cite their sources, and provide valid reasoning based on evidence they claim to have. Otherwise, they are simply propagandists who potentially cause much more harm to our communities than they realise."
Citations
[1] Targownik, L. (2026, June 21). What Oregon can teach Canada about pediatric gender medicine. Data-Driven Transsexual. https://datadriventranssexual.substack.com/p/what-oregon-can-teach-canada-about
[2] Boyd, I., Hackett, T., & Bewley, S. (2022). Prescribing puberty blockers to children: A case of lack of adherence to evidence-based practice and duty of care. Journal of Pediatric and Adolescent Gynecology, 35(2), 234–238.
[3] Bewley, S. (2024). Gender critical practice in obstetrics and gynaecology. BJOG: An International Journal of Obstetrics & Gynaecology, 131(S1), 1–5.
[4] The Detrans Foundation. (2026). Research affiliates and contributors. Retrieved from https://www.detransfoundation.com/
[5] University of Oslo Integrity Committee. (2026, June). Investigation into research misconduct allegations: Waehre, A., Diseth, T. H., & Nyquist, C. B. Integrity Report.
[6] MacKinnon, K. R. (2026, June). The truth about detransitioning. Kinnonrossmackinnon Substack. https://kinnonrossmackinnon.substack.com/p/the-truth-about-detransitioning
[7] Littman, L. (2018). Rapid-onset gender dysphoria in adolescents and young adults: A study of parental reports. PLOS ONE, 13(8), e0202330.
[8] Bauer, G. R., Lawson, M. L., & Morrissette, P. J. (2021). Transgender youth referred to clinics for gender-affirming medical care in Canada. Pediatrics, 148(5), e2020047266. https://doi.org/10.1542/peds.2020047266
[9] Gray, M., Versel, J. L., Mastrangelo, S., Hilal, J., Marr, M. C., & Kittleson, A. R. (2026). Gender-affirming care for transgender and gender-diverse youth in Oregon: Trends over time. Research Connections, 1(2), vmag049. https://academic.oup.com/rescon/article/1/2/vmag049/8657075
[10] @datadriven_tdoc. (June 22, 2026). Everything I've put in there is cited and evidence based [Tweet]. X (formerly Twitter).
[11] @datadriven_tdoc. (June 2026). For natal boys, I have seen much less evidence [Tweet]. X (formerly Twitter).
[12] AllSides Media Bias Chart. (2026). National Post bias rating and analysis. Retrieved from https://www.allsides.com/; Media Bias/Fact Check. (2026). National Post. Retrieved from https://mediabiasfactcheck.com/national-post/
[13] American Psychological Association. (2015). Guidelines for psychological practice with transgender and gender nonconforming people. American Psychologist, 70(9), 832–864. https://doi.org/10.1037/a0039906
[14] Turban JL, Beckwith N, Reisner SL, Keuroghlian AS. Association Between Recalled Exposure to Gender Identity Conversion Efforts and Psychological Distress and Suicide Attempts Among Transgender Adults. JAMA Psychiatry. 2020;77(1):68–76. doi:10.1001/jamapsychiatry.2019.2285
[15] Costescu, D., Massarella, C., Powers, W. J., & Singh, S. S. (2024). A Gender-Affirming Approach to Contraceptive Care for Transgender and Gender-Diverse Patients. O&G open, 1(1), e003. https://doi.org/10.1097/og9.0000000000000003
[16] Nguyen, T. N., Jackson, W. E., Roth, N. C., Cinque, F., Sarkar, M., Samala, N., Lee, R. S., Strauss, A. T., Wisocky, J., Patel, K., Sebastiani, G., Streed, C. G., Jr, Lake, J. E., & Lee, T. H. (2026). Chronic liver disease and hepatology care in transgender and gender diverse populations. The lancet. Gastroenterology & hepatology, 11(4), 334–344. https://doi.org/10.1016/S2468-1253(25)00287-0
[17] College of Physicians and Surgeons of Manitoba. (2020, March 5). Censure: IC4235 - Dr. Laura Targownik. [Disciplinary Record].https://www.cpsm.mb.ca/assets/Discipline/20200305TargownikCensure.pdf
[18] Viana, D. P. C., Câmara, L. C., & Alto, L. S. M. (2026). Cardiovascular mortality associated with testosterone therapy in cisgender women and transgender men: A systematic review. Frontiers in Endocrinology, 17, 1789504. https://doi.org/10.3389/fendo.2026.1789504
[19] Ben Ryan. (2026). Oregon's demographic shift in gender medicine [Report]. Hazard Ratio Substack. Retrieved from https://archive.ph/o/APLyg/https://benryan.substack.com/
[20] Tordoff, D. M., Wanta, J. W., Collin, A., Stepney, C., Inwards-Breland, D. J., & Ahrens, K. (2022). Mental health outcomes in transgender and nonbinary youths receiving gender-affirming care. JAMA Network Open, 5(2), e220978. https://doi.org/10.1001/jamanetworkopen.2022.0978
[21] Turban, J. L., King, D., Kobe, J., Reisner, S. L., & Keuroghlian, A. S. (2022). Access to gender-affirming hormones during adolescence and mental health outcomes among transgender adults. PLOS ONE, 17(1), e0261039. https://doi.org/10.1371/journal.pone.0261039
[22] Targownik, L. (Host). (2026, February 10). Agree to Disagree About Gender - Episode 6: A Conversation with Ben Ryan [Video podcast episode]. YouTube. https://www.youtube.com/watch?v=jPQblLLiD_U&t=342s (for timestamp 5:42)
[23] Lagrange, C., Soutrel, A., Delvenne, V., Cools, M., & Bax, P. (2024). Clinical profiles and care of transgender children and adolescents who attended a French gender identity clinic. Child and Adolescent Psychiatry and Mental Health, 18, 132. https://doi.org/10.1186/s13034-024-00809-w
[24] Testa, R. J., Habarth, J., Peta, J., Balsam, K., & Bariola, E. (2021). Factors associated with age of presentation to gender-affirming medical care. Pediatrics, 147(4), e2020026674. https://doi.org/10.1542/peds.2020-026674
[25] Serano, J. (2023). Explaining assigned sex ratio shifts in trans children. Medium. https://juliaserano.medium.com/explaining-assigned-sex-ratio-shifts-in-trans-children-12c6d01903a3
[26] Vandendriessche, C., Claes, L., Verhulst, B., & Claus, J. (2025). Social factors behind the AFAB predominance in LGBT youths. European Child & Adolescent Psychiatry, 34, 1–12. https://doi.org/10.1007/s00787-024-02595-4
[27] deMayo, B.E., Gallagher, N.M., Leshin, R.A. and Olson, K.R. (2025), Stability and Change in Gender Identity and Sexual Orientation Across Childhood and Adolescence. Monographs Society Res Child, 90: 7-172. https://doi.org/10.1111/mono.12479
[28] Bustos, V. P., Bustos, S. S., Mascaro, A., Del Corral, G., Forte, A. J., Ciudad, P., Kim, E. A., Langstein, H. N., & Manrique, O. J. (2021). Regret after Gender-affirmation Surgery: A Systematic Review and Meta-analysis of Prevalence. Plastic and reconstructive surgery. Global open, 9(3), e3477. https://doi.org/10.1097/GOX.0000000000003477
[29] Serano, J. (2023, March 19). All the evidence against transgender social contagion. Medium. Retrieved from https://juliaserano.medium.com/all-the-evidence-against-transgender-social-contagion-f82fbda9c5d4
[30] Martin, M. (2021, December). Feature: Study dispels harmful gender dysphoria myth. Schulich School of Medicine & Dentistry, Western University. https://www.schulich.uwo.ca/about/news/2021/december/feature_study_dispels_harmful_gender_dysphoria_myth.html
[31] Targownik, L. (2026, April). Unfin(n)ished Business: What the Finnish Register Study Can and Cannot Tell Us About Mental Health in Gender-Dysphoric Youth. Data-Driven Transsexual Substack. https://datadriventranssexual.substack.com/p/unfinnished-business-what-the-finnish
[32] Saunders, R. (2026, July 4). Dear LGBTQI+ community, we need to talk about evidence. Medium. https://rejserin.medium.com/dear-lgbtqi-community-we-need-to-talk-about-evidence-65ca7caff81b
[33] Targownik, L. (2026, April 30). They have a preferred outcome, and they selectively promote narratives and evidence that seek to eliminate one particular modality of care for gender-distressed youth [Twitter post]. Twitter. https://x.com/datadriven_tdoc/status/2049961879834132859



